
Spiral - Spin - Momentum - Want
The House We All Live In: A Framework for Emotional Navigation Beyond Diagnosis
By Pauline Pearson | Mental Health Social Worker & Psychotherapist, Melbourne
This article was originally published in Italian in Mad in Italy, March 2026. This is the original English text as submitted by the author.
Something Is Missing
I want to begin with a feeling rather than an argument.
It is the feeling — familiar, I suspect, to many people who work in mental health — that something important is not quite being reached. That the frameworks we have, for all their genuine achievements, leave a particular kind of human experience unnamed. Not the dramatic presentations, not the crisis moments, not the clear diagnostic pictures — those are well mapped. I mean the quieter, more pervasive experience of people who know something is happening inside them but cannot find words for it that feel true. People who arrive at their first appointment already wearing a label that arrived before anyone had really listened. People who understand their diagnosis perfectly and still do not know where they are.
I have been a mental health social worker and psychotherapist for thirty years, working across community settings, hospitals, crisis services, and private practice. I also hold a science degree and have spent many years in the study and experience of psychoanalysis. What I want to offer here is not a critique of any of those traditions. It is something that emerged from sitting inside them for a long time — a framework born of paying close attention to what people actually say when they try to describe their inner lives, before the clinical vocabulary has settled over the conversation.
It began with a word.
The Word People Already Use
Listen carefully to someone describing their emotional experience — not in a clinical intake, but in ordinary conversation — and a particular word comes up again and again.
Spiral.
Not anxiety. Not depression. Not mood episode. Just: spiral.
People spiral up into overthinking and panic. They spiral down into withdrawal and the numb flatness where self-care quietly falls away. The word arrives without prompting, across age groups, cultural backgrounds, degrees of distress. It describes not just a feeling but a movement — directional, dynamic, something with momentum that can actually be worked with.
I have come to believe this word points toward something the mental health field has largely passed over: that people already carry within themselves a precise and useful vocabulary for their emotional experience. They have simply never been given a map to go with it.
This article is an attempt to offer that map.
What the Dominant Language Has Given Us — and What It Has Not
The medical model of mental health has given us a great deal. It has given us treatments that work for some people in some circumstances, a shared professional vocabulary, and a framework that has reduced — in some quarters at least — the moral judgement that once attached itself to emotional suffering. These are genuine achievements and I do not want to dismiss them.
But I have watched, across three decades, as the vocabulary of illness and disorder has gradually colonised the whole of emotional life. Anxiety, depression, disorder, diagnosis — these words have become so familiar they no longer feel like a professional framework at all. They feel like reality itself. People arrive at their first counselling appointment already self-diagnosed, having pre-translated their experience into medical language before anyone has listened to it. The label arrives before the person. And once a label is in the room, it is remarkably difficult to hear what was there before it.
The medical model is, at its heart, a model of what is wrong with you. It locates the problem inside an isolated individual unit, classifies it, and implies a treatment delivered by someone more qualified than you to correct the malfunction. This is sometimes exactly right. But it is not always right, and its dominance means there is little room for other kinds of understanding to develop and be funded and taught.
Fritjof Capra observed, decades ago, that the mechanistic, reductionist paradigm of classical science — locate, classify, treat — was giving way in many fields to a systems-thinking understanding of living processes as dynamic, interconnected, and always in motion (Capra, 1982). That shift has been slow to reach mental health. What follows is an attempt to bring it there — not to replace what we have, but to sit alongside it and offer something it cannot quite offer itself.
What the Spiral Actually Tells Us
The spiral is not merely a metaphor. It is a structure that appears throughout the natural world with a frequency that feels almost intentional. It curls in the chambers of a shell and unfurls in the frond of a fern. It sweeps through the arms of distant galaxies and tightens in the eye of a hurricane. DNA — the molecule at the very core of life — is structured as a spiral. Nature returns to this shape again and again because it is one of the most practical available: it allows a living thing to keep growing at its outer edge while its essential form remains whole and recognisable.
More recently, neuroscience has found the spiral moving through our inner worlds as well. Research from the University of Sydney has demonstrated that the brain produces spiral-shaped waves of electrical activity — rotating patterns that appear to play a role in how different regions communicate, in the rhythms of sleep, and in how we process emotion and experience (Xu et al., 2023). The spiral, it seems, is not just a poetic description of how emotional life moves. It may be something closer to a literal one.
We are not broken. We are people in motion. And motion — unlike malfunction — can be understood, anticipated, and gently redirected.
Consider a ball on the end of a string, spinning in the air above your head. Speed up the rotation and the ball rises, vibrating at a higher frequency. Slow it down and it descends, the frequency dropping, the motion becoming heavier and slower. It is always in motion. The direction can change. But direction does not change by itself — it changes when the forces acting on the system change. Momentum is real. It has to be worked with, not overridden.
I have come to think this is a more honest description of emotional life than most of what appears in clinical manuals. We do not simply toggle between well and unwell. We move — through states that are genuinely different from one another, each with its own frequency, its own way of perceiving the world, its own sense of what is possible and what is not. Anyone who has lived through a panic attack and then the exhausted flatness that sometimes follows will recognise this immediately. These are not just different moods. They are different speeds of the whole self — body, nervous system, mind, and perception together.
The House Within
What if we built a map of the inner world using the spiral as its organising principle? Not a diagnostic map that classifies people, but a navigational one — something anyone could learn to read, that belongs to everyone who lives an emotional life, which is to say everyone.
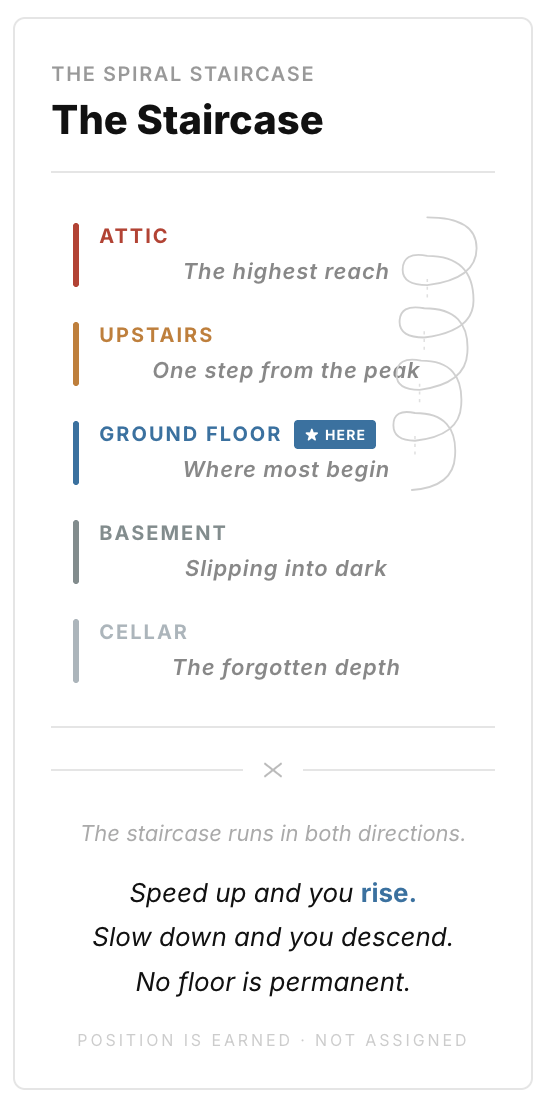
This is the essential claim of The House Within: that the territory it describes is universal. Every human being who has ever lain awake at three in the morning with a racing mind, or felt too heavy to get out of bed, or found themselves snapping at someone they love before quite understanding why — every one of us already lives in this house. Your House Within and mine are the same: five floors, connected by a spiral staircase.
The Ground floor deserves particular care in its description, because it is frequently misunderstood. It is not a state of perfect calm. It is not happiness, or the absence of pain, or the performance of equanimity. On the Ground floor, you can feel angry, sad, frightened, or deeply worried. The full range of human emotion is present and available here. What is different is what you can do with those feelings. Emotion and thought can coexist on this floor. You can feel something strongly and still hold it — still bring your capacity to think clearly, to consider others, to ask what response will genuinely serve the situation rather than simply relieve the pressure inside you. This is the floor of purpose — where we act from what we value, not just from the momentum of the moment.
One more thing belongs exclusively to the Ground floor, and it is worth stating plainly: gratitude and compassion are only authentically available here. On the upper floors, spinning with anxiety or overwhelm, there is no real room for them — the frequency is too high, the focus too narrow. On the lower floors, collapsed in withdrawal or enclosed in the defended world of the Cellar, they cannot take root either. They arise naturally on the Ground floor, and only there. This is not a moral prescription. It is a description of what these floors make possible.
The Upstairs is where emotional momentum begins to carry us higher. The mind accelerates into overthinking, over-worrying, over-stressing. We begin to forecast catastrophe without data — constructing vivid, detailed pictures of the worst possible outcome and treating them as facts about the future rather than fears about it. Many people spend long stretches on the Upstairs floor, so habituated to its particular hum that it no longer feels like a heightened state. It simply feels like what a responsible person should feel.
The Attic is further still — spinning faster, vibrating at higher frequency. Daniel Siegel's Window of Tolerance (1999) calls this zone hyperarousal, and the description is accurate: this is the floor of explosion and overwhelm, where the body overrides the mind entirely. We erupt, or we freeze. Panic lives here. The Attic has its own evolutionary logic — in genuine danger, it serves us magnificently. The difficulty is when we arrive there in response to an email.
The Basement is the first floor below ground, and it carries a different quality entirely. Where the Attic is frantic, the Basement is slow and heavy — the frequency has dropped, and with it the sense of possibility. Siegel's third zone — hypoarousal — lives here. This is the floor of the inner voice that turns against itself: poor me, nothing ever works for me, what is the point of even trying? The world is seen through the lens of lack. Everyone else seems to have what I feel I do not. This is not weakness or failure. It is a state of mind with its own gravity, pulling thought in a particular direction, and it deserves to be met with curiosity rather than judgement.
The Cellar is the deepest floor, and it extends Siegel's model into territory his three-zone framework does not fully reach. It is not primarily a place of sadness. It is a retreat into a defended, self-enclosed world in which only one's own immediate desires matter — the organising principle being, essentially, if I want to do it, I will do it, regardless of whether it harms me or anyone else. Addictions live on this floor. So does the emotional game-playing — manipulation, deflection, the performance of helplessness or invulnerability — that keeps genuine contact with other people at arm's length. The Cellar is not a moral judgement. It is a location on a map. And the most important thing a map can tell you about any location is that it is not permanent.
Ask anyone — a teacher, a tradesperson, a grandparent, a teenager, a psychiatrist — and they will recognise every floor from their own life. We differ in which floors we favour and how long we tend to stay. But we have all been on all of them. The house is not a clinical invention. It is a description of shared human experience, finally given a name.
Where These Ideas Come From
I want to say something about the intellectual roots of this framework, because they are more diverse than a clinical paper might typically acknowledge — and I think that diversity is itself part of what the framework is trying to say.
The spiral as an organising principle draws, as described above, on both the natural sciences and recent neuroscience. But it also draws on traditions of thought that have been attending to the physics of inner life for a great deal longer than Western clinical psychology has existed.
Buddhist psychology describes the mind in terms of states that arise and pass — not fixed conditions but dynamic movements, each with its own character, each inclining toward the next. The teaching is not "what caused this state?" but "what is the nature of this state, and what does it tend to generate?" The emphasis is always on present-moment recognition rather than historical excavation. The five floors of The House Within are recognisable in this light as a map of arising and passing states, each with its own frequency, each with its own kind of suffering and its own kind of wisdom.
Vedic traditions have for millennia described experience in terms of prana — life energy moving through the body at different frequencies and densities — and of states of consciousness that correspond to different vibrational levels. The Vedantic concept of gunas — the three qualities of tamas (heaviness, inertia), rajas (activity, agitation), and sattva (clarity, balance) — maps with striking directness onto the floors of the House Within. The Basement and Cellar carry the quality of tamas. The Upstairs and Attic carry the quality of rajas. The Ground floor — where emotion and thought coexist, where we act from what we value — carries the quality of sattva.
Taoism contributes a third thread, and perhaps the most directly practical one. The Taoist understanding of wu wei — often translated as non-action, but better understood as acting in accordance with the nature of things rather than against them — is exactly the therapeutic logic of working with the spiral. You cannot simply override momentum. You cannot will yourself off the Attic floor any more than you can stop a spinning top by grabbing it. What you can do is understand the nature of the motion, work with the forces acting on it, and allow the direction to change by understanding rather than by force. The Taoist practitioner does not fight the river. They read the current.
These traditions are not cited here as scientific authorities. They are offered as evidence of independent convergence — different cultures, different centuries, different languages, arriving at related insights about the physics of inner life.
Why Spiralling Feels Good — and What to Offer Instead
There is something about spiralling that is rarely said in clinical settings, perhaps because it seems to complicate the work. Spiralling, in both directions, feels good.
The word that comes closest is delicious.
There is a particular pleasure in getting caught up in overthinking and over-stressing — a kind of electric intensity, a feeling of being fully alive to the stakes. There is an equally particular pleasure in sinking into the Basement — in the soft, familiar comfort of nothing ever works for me — a pleasure that is melancholy but real, like a sad song you keep returning to when you could easily choose something else. Or the quiet comfort of a drink, or the numbing pull of a screen.
This matters enormously for practice. Telling people to simply stop spiralling asks them to give up something they are genuinely getting something from — without offering anything in return. The spiral, in both directions, offers feeling at full volume. It is seductive precisely because it is vivid.
The Ground floor offers something different — quieter, less immediate, but I believe more durable. The feeling of having chosen well under pressure. The slow accumulating satisfaction of making real progress toward something that genuinely matters. The particular quality of being the author of your own actions rather than simply their passenger. It is less loud than the spiral. But once a person has really experienced what the Ground floor offers — not as an idea but as a felt reality — the pull of the spiral begins, gradually, to lose some of its authority.
We have a choice. Not because choosing is simple, or because willpower is sufficient, or because the spiral does not pull hard. But because understanding where we are is the beginning of being able to move.
The Space Between People — and What No Diagnosis Can Reach
There is something this framework can do that I have not found another clinical tool quite managing: it can help us understand the space between people, not just the interior of one person considered in isolation.
A diagnosis is about one person and their ill health. It says nothing about what is happening between two people — why a conversation went wrong, why a client's distress pulls a clinician into their own, why certain relationships seem to trap both people in the same unproductive loop. It has no language for the way one person's emotional floor calls to the floors of everyone around them.
The House Within does. Because every person in a relationship — a child, a parent, a partner, a colleague, a client — has their own House Within with the same five floors. Once we understand the map, we can begin to see not just where we are, but which floor the people around us are on. And that changes everything about how we respond.
Floors are contagious in ways we rarely acknowledge. When a client is speaking from the Basement — lost in the quiet conviction that nothing works, that everyone else has what they lack — they are extending an invitation, often unconsciously, for us to join them there. We cannot move someone else along their spiral staircase. What we and only we can control is which floor we are on in our own house. But that turns out to matter more than almost anything else. If a client is in the Attic — overwhelmed, panicking, unable to think — and we meet them from our own Attic, the frequency in the room doubles. If we can stay on our Ground floor, we offer them something they cannot give themselves in that moment: the steadying presence of someone who is not spinning.
A Framework for Everyone
The House Within is designed to teach, not to diagnose. The word doctor derives from the Latin docere — to teach. It is one of medicine's oldest self-descriptions, and one it has largely set aside.
We teach people to drive and to swim. We distribute knowledge about fire safety, road safety, sun safety — understanding that practical knowledge distributed widely builds populations of people who can recognise risk, respond with competence, and reduce the demand for crisis intervention. We do not do this for emotional life. The medicalisation of inner experience has made it structurally difficult to do so — diagnosis and treatment are individual, private acts that cannot be scaled to communities or delivered in classrooms.
The House Within can be. It can be introduced to children learning about their emotions in school, to parents trying to understand their own reactivity, to teachers navigating a distressed classroom, to workers in aged care, disability services, refugee programmes, and sporting clubs. Because it requires no diagnostic threshold to be useful, it belongs to anyone willing to pay attention to the movement of their own inner life — which is to say, it belongs to everyone.
In Closing
Last year a client in her early fifties — a senior manager, capable and experienced and thoroughly accustomed to finding her way through difficult things — sat across from me and said: "I know something is happening inside me but I don't have the words for it. All I know is I haven't felt like myself in a long time."
She was not unwell. She was lost. And what she needed was not a diagnosis.
It was a map.
This is what I hear again and again, across very different people and very different circumstances. Not confusion about symptoms. Confusion about location. People know something is happening. They do not know where they are, or how they got there, or which direction leads back toward the person they recognise as themselves.
The House Within gives people that orientation. And because it is built around the word they were already using — because it names something they already knew — it does not feel like something imposed from outside. It feels like recognition.
That, I think, is what the best vocabulary does. It does not change the experience. It makes the experience navigable. And what we can navigate, we can begin to work with.
The house has always been there — in every person who has ever spiralled upward into panic, in every person who found themselves in the Cellar and wondered quietly how they got there, in every person who has stood on the Ground floor and felt the quiet, particular relief of being able to think clearly and choose well.
We all live here. We always have.
It is time we gave each other a proper map.
Pauline Pearson is a mental health social worker and psychotherapist based in Melbourne, Australia, with thirty years of experience across community, clinical, and crisis settings. She holds qualifications in social work, science, and psychoanalytic psychotherapy. She is the developer of The House Within framework for emotional education and literacy.
References
Brackett, M. A., Rivers, S. E., & Salovey, P. (2011). Emotional intelligence: Implications for personal, social, academic, and workplace success. Social and Personality Psychology Compass, 5(1), 88–103.
Capra, F. (1975). The Tao of physics: An exploration of the parallels between modern physics and eastern mysticism. Shambhala Publications.
Capra, F. (1982). The turning point: Science, society, and the rising culture. Simon & Schuster.
Deegan, P. E. (1996). Recovery as a journey of the heart. Psychiatric Rehabilitation Journal, 19(3), 91–97.
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton & Company.
Siegel, D. J. (1999). The developing mind: How relationships and the brain interact to shape who we are. Guilford Press.
Snyder, C. R. (2002). Hope theory: Rainbows in the mind. Psychological Inquiry, 13(4), 249–275.
Xu, Y., Long, X., Feng, J., & Gong, P. (2023). Interacting spiral wave patterns underlie complex brain dynamics and are related to cognitive processing. Nature Human Behaviour, 7, 1196–1215. https://doi.org/10.1038/s41562-023-01626-5